
U.S.

At the end of this year, the targets set by the United Nations in 2000 for developing countries will expire. In this project, we take those Millennium Development Goals and examine how some communities in the United States measure up. We have applied each goal to the U.S. by looking at an indicator used to measure a country’s development success and interpreting it for a specific community in America. The eight goals are: eradicate extreme poverty and hunger, achieve universal primary education, promote gender equality and empower women, reduce child mortality, improve maternal health, combat HIV/AIDS and other diseases, ensure environmental sustainability, and develop a global partnership for development. An indicator for the eighth goal — develop a global partnership for development — is the proportion of population with access to affordable, essential drugs on a sustainable basis. In this piece, we explore the impact of the United States’ extremely high cost of health care and medication in Texas, the state with the largest uninsured population.
LUBBOCK, Texas — Teianna Mitchell was so desperate to make money last summer that she found herself wading through college students’ trash and scrubbing their toilets to make their apartments look new after they moved out of their student housing.
“They didn’t give us enough supplies, and some of those apartments were filthy,” she said, laughing as she remembered the short-term job she found on Craigslist — a job she took so she could afford her medicine. “One time there was even a used condom left on the floor. It was the worst thing ever. It was such a humbling experience.”

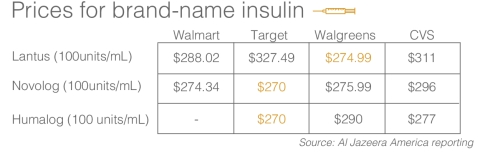
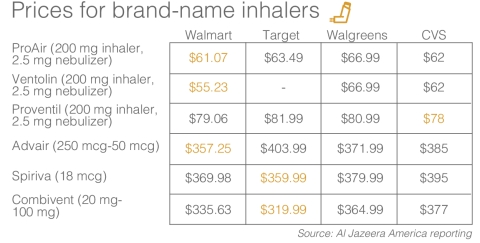
Mitchell, now 20, was diagnosed with Type 2 diabetes when she was 16. She regularly takes insulin through a pod, and she occasionally uses an inhaler to treat her chronic asthma. She used the $240 she earned from the cleaning job to repay her mother, who had lent her money when she had run out of insulin and cash.
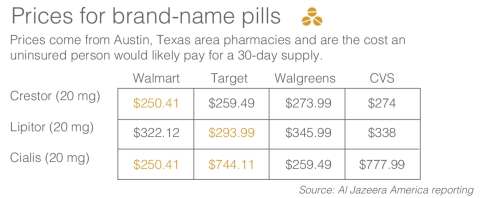
She spends close to $600 each month on her prescriptions and supplies to manage just her diabetes. And in Texas, despite the fact that she struggles to afford her prescribed medications, she’s still one of the fortunate ones, because she is insured.
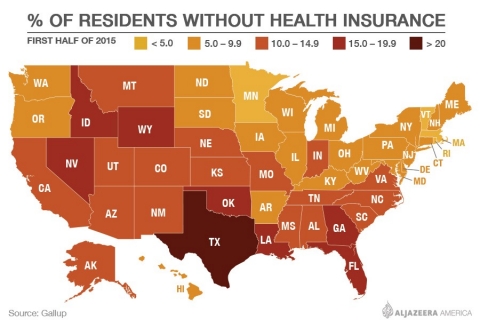
Different surveys tell you different stories about being uninsured in Texas. Data from the Centers for Disease Control and Prevention indicate that as of June 2015, 21.6 percent of Texans are uninsured; a Gallup survey through the middle of this year put the uninsured rate at 20.8 percent. A study released in March 2015 by the Episcopal Health Foundation and Rice University’s Baker Institute for Public Policy marked a nearly 8 percentage point drop in the uninsured rate in Texas since the Affordable Care Act went into effect in late 2013, to 16.9 percent.
But all these studies agree that Texas leads the nation with the highest percentage of uninsured people. And the Episcopal Health Foundation and Baker Institute study noted, “For the first time, Texas now has the largest number of uninsured residents.”
Cindy Mathis, a 38-year-old single mother of four, is one of them. Her three youngest children still live at home and are all insured. The two youngest are even double insured, she said, because when she filled out the paperwork for Medicaid — a step she was told to take while trying to sign up for coverage through the Affordable Care Act — they qualified. But because she receives child support in addition to her $19,000-a-year salary, she does not.
She chose to go without health insurance.
“I pay out of pocket for everything, and it is cheaper for me to do that than it is for me to pay the insurance the government is forcing me to try to get,” she said, referring to the Affordable Care Act’s financial penalty for those who go without insurance.
“The cheapest insurance that they can offer me in the marketplace you go to online is $190-something dollars a month just for myself. I’d have to pay a $6,000 deductible, and all I take is a birth control pill every month.”
Mathis is lucky too, but only in the sense that she is healthy and can, for the time being, afford to be uninsured — even when she gets sick.
“During the summer I got a respiratory infection, and I had to pay $85 out of pocket for an inhaler because I didn’t have insurance, after paying $60 cash to go to the doctor,” she said. While the trip to the doctor wasn’t planned, she said she has gotten by so far by putting pencil to paper and budgeting her health care costs. She said she spends less than $400 a year on doctor visits and medication, including an annual trip to the gynecologist for her and to the dentist and eye doctor for her kids — and one “sick visit.”
“Now, if I start having blood pressure issues or high cholesterol or something like that, I’m going to be in trouble because I’m not going to be able to afford the medication,” she said.

But while researchers have a pretty good idea of how many Texans are uninsured, Amanda Jovaag, the lead data researcher for the University of Wisconsin at Madison’s county health ranking project, said that there haven’t been studies on how many people can afford their prescribed medications.
“But we do know that insurance is an important barrier to all kinds of care — primary care, mental health care and, one would assume also, prescription drug coverage,” she said. “In general, the principle certainly has proven true in our research and in other people’s research.”
The health ranking project measures the health of nearly every county in the country and ranks those counties in their state by looking at factors like tobacco and alcohol use, access to and quality of care, education, employment, income and the quality of a county’s air and water.
Mathis lives in Shelby County, which hugs the border with Louisiana, deep behind the pine curtain in East Texas. According to the 2015 county study (which uses data from 2010 to 2012), 6,513 Shelby residents under the age of 65 — or 30 percent of the population — are uninsured.
She said at least half the people she knows well have trouble paying for their health care coverage and prescription costs. A Texas pharmacist who works for a national chain estimated that 10 to 15 percent of her regular customers are uninsured and that 20 to 25 percent of her insured customers have trouble paying for their prescriptions. She spoke on condition of anonymity because her company doesn’t allow employees to speak to the press.
There are avenues that can help.
The first, the pharmacist said, is to call patients’ doctors and ask if generic drugs can be prescribed rather than name brands, which are more expensive. Many chain pharmacies, including those at Walmart, Target, and Walgreens, offer generic medication lists; 30-day supplies of generic prescribed drugs on the lists are sold for a small fee, typically $4, regardless of whether a patient is insured; 90-day supplies usually cost $10.
If a generic drug won’t do, some patients turn to the Internet in search of prescription discount cards. These cards work exactly as they sound — they offer discounts at pharmacies for prescriptions — but the pharmacist said that they don’t compare with having insurance.
A third and perhaps most effective way to get cheaper prescriptions is to use what pharmaceutical companies call prescription assistance programs, such as Texas’ free statewide Texas Drug Card, which connect patients with pharmaceutical companies or third parties that offer prescriptions at a heavily discounted prices — often free or nearly free.
One of the biggest prescription assistance programs nationally is the Partnership for Prescription Assistance (PPA), a program sponsored by 16 Pharmaceutical Research and Manufacturers of America (PhRMA) member companies. Since its inception in 2005, the PPA has served 9.5 million Americans — 434,888 of them Texans.
The programs work differently, depending on the drug and the pharmaceutical company or third-party provider that can provide it. Some send a supply of medicine straight to a patient’s home, while others provide a voucher or coupon for a patient to take to a pharmacy. But programs like the PPA are avenues being used not just by customers who are uninsured, because affordability comes down to more than the list prices of medicines, said Holly Campbell, the communications director for PhRMA.
“A patient may have insurance, but a lot of insurance benefit designs now have four or five tiers, so patients are no longer being asked to perhaps pay a copay if they go to the pharmacy for their medicine but now a coinsurance, which is like a percentage of a medicine price that the insurance sets,” she said.
It’s a design that she said makes prescription access affordable for fewer and fewer people. Covered medication is divided into tiers on a formulary determined by each insurance company. Drugs found in tiers 1 and 2 are cheaper and typically generic. If a patient requires step therapy — when a medicine in a lower tier doesn’t work and a patient must be prescribed a drug in a higher tier — a patient will see coinsurance costs rather than a set copay.
If a drug is left off a formulary or if an insurance company determines that a patient doesn’t qualify for coverage, it’s up to patients to pay for the medicine or work with their insurance company to try to get the drug included on the formulary. In some instances, patients, like those needing new hepatitis C drugs, are looking at price tags upward of $60,000 — prices prohibitive to receiving the care they need.
And in at least one recent instance, those costs were deliberately passed along to patients. Pharmaceutical company CEO Martin Shkreli was arrested on Thursday and charged with securities fraud and wire fraud after becoming a notorious figure in price-gouging scandals, mostly notably for acquiring a decades-old drug and increasing its price by 5,000 percent overnight.
Mitchell’s costs aren’t that prohibitive yet, and she reminds herself that she is blessed to have insurance. Still, she said her life would look very different and she would have more options if she didn’t have to pay for all those prescriptions. As it is, she lives rent-free at home and has two classes left at South Plains College to finish her associate’s degree in graphic design. Because she’s paying for school through FAFSA grants and her father’s GI Bill benefits, after she completes her associate’s degree, she will continue to live in Lubbock and complete her education close to home.
“If I didn't have any health costs, I would move out in a heartbeat, to Portland or Santa Fe, whichever city had the nicest design school I could attend to get my bachelor’s degree,” she said. “But I don’t think I can move out until I get a career. I can’t go completely broke. My health depends on it.”

In part 1 of our ‘America left behind’ series, Al Jazeera looks at a community where 1 in 3 is diabetic or at risk
In part 2 of our ‘America left behind’ series, Al Jazeera explores the vicious cycle of poverty and lack of education

In part 3 of ‘America left behind,’ Al Jazeera explores why the US trails many developing nations in electing women

As part of the ‘America left behind’ series, Al Jazeera looks at the high black infant death rate in the Magnolia State

In part five of ‘America left behind,’ Al Jazeera explores why the US is failing to reduce its maternal death rate

In part 6 of ‘America left behind,’ Al Jazeera looks at why 37 states teach abstinence despite evidence it doesn’t work










Error
Sorry, your comment was not saved due to a technical problem. Please try again later or using a different browser.