
Health
John Moore / Getty Images
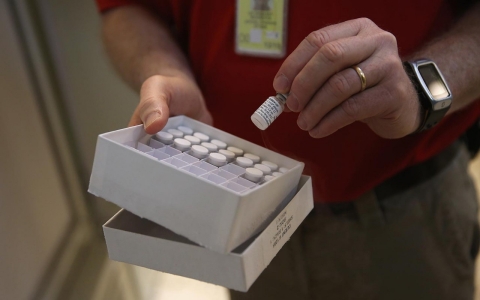
FREETOWN, Sierra Leone — Since Ebola hit this coastal city last summer, nurses at Connaught Hospital have put their lives on the line by working with patients at risk of the deadly disease. Now researchers aim to recruit them as well as ambulance drivers and other hospital staff as subjects in one of the largest Ebola vaccine trials to date.
But just a few weeks before the trial begins enrollment, many health care workers are voicing discomfort about the shot. “It would be really good to have a vaccine, but we’re scared because it’s new,” said Kadiatu Nubieu, a nurse at Connaught.
Researchers say the vaccines are safe, on the basis of small studies last year in which recipients did not suffer major side effects. Now researchers are planning for the final phase of trials designed to determine the efficacy of the vaccines. Health workers such as Nubieu are ideal study participants for these trials because their chances of infection are higher than for members of the general public. If a vaccine keeps them healthier than unvaccinated hospital staff, scientists will have confidence in their product.
In the coming weeks, researchers plan to enroll 6,000 to 8,000 health workers in a trial in Sierra Leone, supported by local researchers, the U.S. Centers for Disease Control and Prevention (CDC) and the Merck pharmaceutical company. As the team scrambles to launch the trial before the outbreak ends, they are compressing certain steps, including outreach to potential participants.
Several health workers in Sierra Leone said they feel overlooked in a process that intimately affects their lives. “I’m not sure whether or not I’ll take the vaccine,” said William Bangura, a nurse working in the Ebola isolation unit at Connaught. “I want to know why no CDC person has ever met us here to talk.”
The CDC says it plans to meet directly with health workers a couple of weeks before the trial’s start. But if nurses’ sentiments around Freetown are any indication, building trust between the agency and hospital staffers may take more effort than scientists expect.
“Communication is one of the most important things to concentrate on,” said a researcher not involved with Ebola vaccines, David Diemert, the director of clinical trials at the Sabin Vaccine Development Partnership in Washington, D.C. He conducted several trials for vaccines in the developing world and said good communication “can make or break a program.”

Scientists expected Ebola vaccine development to take time. The research began more than a decade ago after outbreaks in the jungles of the Democratic Republic of Congo. Because the Ebola virus is so lethal, killing most of its victims within a few weeks, researchers realized the vaccines would be more complicated to construct than those for measles, flu or polio. Those shots rely on weakened or dead versions of the pathogens underlying the diseases, which then trigger the slow production of antibodies that stop subsequent infections.
Scientists dared not take chances with weakened or killed versions of the Ebola virus. Instead, they spent years engineering molecules that consisted of a single gene from Ebola, attached to a harmless virus that could carry the gene through a person’s bloodstream and into their cells, where it would trigger the production of Ebola antibodies.
Some researchers attached the Ebola gene to viruses that cause colds in chimpanzees, a type of adenovirus. Canadian scientists bound it to a cattle virus called VSV (for vesicular stomatitis virus). From 2000 to 2005, monkeys injected with versions of the adenovirus and VSV vaccines generated Ebola antibodies. In the years that followed, studies found that some vaccinated monkeys were protected against the disease. These were good signs, but the research more or less froze there. Clinical trials cost millions of dollars, and neither public organizations nor pharmaceutical industries were willing to invest money when it was not clear whether the shots would ever hit the market.
That changed soon after Aug. 8, 2014, when the World Health Organization declared Ebola an international emergency. At that point, more than 1,779 people had been infected with the virus, and over half had died. To stimulate research on the shelved shots, the U.S. government agreed to partner with West African scientists and pharmaceutical companies. Then the real work began.
From November to January, small trials on the adenovirus and VSV Ebola vaccines in the U.S., the U.K., Switzerland, Canada, Germany, Mali, Kenya and Gabon showed that people given the shots did not develop life-threatening side effects in the weeks that followed. In January a 600-person placebo-controlled trial designed to assess the safety of the adenovirus and VSV Ebola vaccines as well as the buildup of antibodies was slated to launch in Liberia.
The team was delayed, however, because potential study participants were uneasy, said Fatorma Bolay, director of the Liberian National Institute for Biomedical Research and one of the study’s lead researchers. He decided to step up his team’s outreach in the community where they hoped to enroll participants. For weeks, the researchers walked from house to house to discuss the vaccine and tests they had done on its safety. By the time the study began in February, they had plenty of volunteers.
“The advice I give my colleagues is to not get frustrated when you are asked the same questions over and over again,” he said. “If people are asking, it means that you have failed to get your message across and you need a better strategy to get to the people so they understand.”
By early March, Bolay and his team had enough data to give them confidence that the vaccines caused no major problems. But the final study — the large and long-term one to determine whether the vaccines prevent Ebola — has met another obstacle in Liberia: On March 5, the last Ebola patient in the country was discharged.
By default, the spotlight now shifts to Sierra Leone, which has accounted for two-thirds of the world’s cases in the past few weeks. There the study testing the efficacy of the VSV vaccine in nurses, ambulance drivers and other hospital workers has been in the making since November. Initially, researchers expected it to start in January, but it has yet to launch.
After receiving approval from two Sierra Leonean review boards, the CDC and the U.S. Food and Drug Administration, the team now awaits one final go-ahead from the pharmacy board in Sierra Leone.
Urgency is palpable as the outbreak ebbs. Unless a few dozen people in the control arm of the trial end up contracting Ebola, there’s no proof that the vaccine has fended off the disease, said Daniel Feikin, an epidemiologist with the CDC and an investigator on the study.
Although the VSV vaccine was reasonably safe in earlier studies, there remains some concern that people with undiagnosed immune system problems, such as HIV, could suffer adverse reactions to the shots. The team pledges to catch and treat these responses immediately. But their promise means less to some nurses than a demonstration of the vaccine’s safety. Specifically, health workers have asked the investigators to enroll in the study themselves. Study investigators do not typically participate in trials, and this one will be no exception for CDC staff. Agency employees say they do not qualify for the study since they do not reside in Sierra Leone.
However, Baimba Idriss, a young local doctor who will help run the vaccine trial at 34th Military Hospital in Freetown, understands the strength of people’s suspicions. A well-known figure because of his work fighting the disease — he treated the first Ebola patient in Freetown and dozens thereafter — he plans to enroll in the trial in an effort to allay the public’s concerns. “I’ll get the vaccine to help convince people that it’s safe,” he said. “If I am the first to do it, many people will follow.”

While awaiting the green light, Feikin and his team have announced the trial on the radio, called a press conference and met with government and area leaders. But they have yet to speak directly with the hospital workers they hope to include when the study begins in late March. “We want to talk with health care workers within a couple of weeks of enrollment so that the knowledge is fresh in their minds,” he said.
That leaves the team a much shorter time frame for communication compared with other vaccine studies in the developing world. For example, researchers involved in a trial in Brazil on an experimental hookworm vaccine spent a year educating the community before they launched. “We used various techniques — videos, theater, talks with community leaders — in addition to face-to-face meetings,” said Diemert, an investigator on the study. Those conversations paid off.
During the trial, some participants suffered allergic reactions to the hookworm vaccine. Diemert feared that the scientists would be run out of town. Instead “[the community] said, ‘You had warned us of these risks, and you took good care of us when it did happen, and we will continue to participate in trials,’” he said. “I’m convinced that’s because we spent so much time preparing the community.” The time they spent on communication not only educated people but also built trust, he said.
In Sierra Leone, the public’s lack of confidence in the vaccines runs deeper than the science involved. In part, the skepticism is rooted in a history of unfulfilled promises. Roads built by mining companies have eroded within a single rainy season, donated ambulances arrived in the capital months after Ebola ravaged the city, and health workers’ salaries frequently go missing.
Standing outside the Ebola isolation unit at Connaught Hospital, triage assistant Alieu Sesay said, “I’m discouraged because I haven’t gotten my pay. We’re unappreciated, and now they want to test things on us.”
This story was supported by a grant from the Pulitzer Center on Crisis Reporting.

Twenty volunteers immunized in the US all produced antibodies, according to Ebola vaccine researchers

As children who had been declared Ebola-free come down with the disease, this 17-year-old takes on their care










Error
Sorry, your comment was not saved due to a technical problem. Please try again later or using a different browser.