The browser or device you are using is out of date. It has known security flaws and a limited feature set. You will not see all the features of some websites. Please update your browser. A list of the most popular browsers can be found below.
Triina, in a bar in Mahnomen, Minnesota.
Jolene Yazzie for Al Jazeera America
WHITE EARTH RESERVATION, Minn. — She smokes cigarettes constantly. Her fingernail polish is flaking. She lives with her aunt and has pictures of Jesus on her walls. She wipes a spot of blood from her arm and drops a used needle into a red container embellished with a bright orange sticker bearing a biohazard symbol. Triina, 25, is an Ojibwe tribal member and was born and raised on the White Earth Reservation.
“I used to go hard and stay high for days and days,” said Triina, who agreed to be interviewed if her real name wasn’t used. “I don’t do it as much, and I don’t go as hard, and I don’t run like I used to. My body is not what it used to be.”
She crossed her legs on the edge of her bed and lit a cigarette, unsatisfied with her high. She couldn’t get her hands on heroin, her favorite drug, and settled for mainlining meth in the meantime. For Triina, drugs — from cocaine to heroin — can cost her a couple of hundred dollars a day.
“I do want to quit, and I am going to quit. I just don’t know when,” she said. “I don’t want to say, ‘I promise in three or four months I’m going to be sober,’ but hopefully I don’t OD before then, because the reality of this whole thing is always that.”
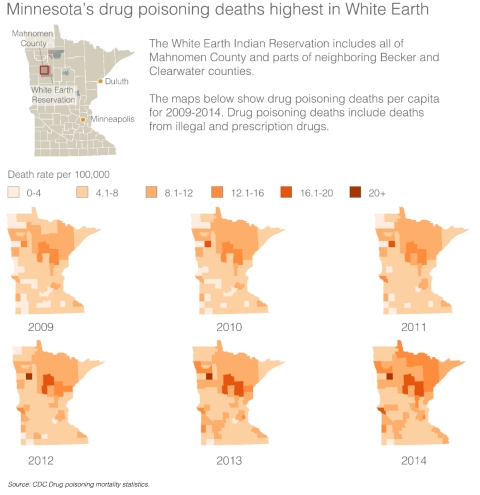
From 2007 to 2009, Native Americans died of drug overdoses at twice the rate of the general U.S. population. From 1999 to 2013, the number of Native Americans who died from drug overdoses increased fourfold. Last year nearly 11,000 patients at Indian health care facilities were diagnosed with opioid use disorder.
“We are seeing increases in heroin at some places across the nation, on reservations,” said Charles Addington, the deputy associate director for the division of drug enforcement for the Bureau of Indian Affairs (BIA). “It’s not completely across every reservation in the U.S., but it’s in specific regions and pockets.”
In December the Indian Health Service (IHS) and the BIA announced a new effort to tackle drug overdoses in Indian Country: Across 60 reservations, 340 BIA law enforcement officers on patrol will carry naloxone, a medication capable of reversing opiate overdoses. The IHS also announced that 95 of its pharmacies will start dispensing naloxone as part of the plan.
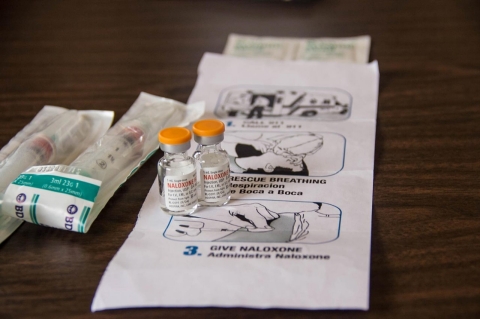
Vials of naloxone with instructions on how to administer it. Jolene Yazzie for Al Jazeera America
Police in 31 states carry naloxone and have documented hundreds of overdose reversals. The drug works by knocking opiates off receptors in the central nervous system and can be administered intravenously or nasally. However, during an overdose, many users stop breathing, so there is often only a small window of time to administer the drug before brain damage occurs.
Health professionals and experts have mixed opinions about the program and its implementation.
“Depending on the particular needs of a particular tribe, I think this could be a useful tool,” said Affie Ellis, a member of the now defunct Indian Law and Order Commission, which was charged with assessing whether the criminal justice system in Indian Country is working or failing. “But to look at it as a magic wand or a silver bullet would be a mistake.”
Because of staff shortfalls, expansive rural patrol areas and chronic underfunding, police presence in Indian Country is often slim to nonexistent. Approximately 362 reservations sit on more than 56 million acres of Indian land in the United States. The Navajo Nation, the largest reservation in the United States, is roughly the size of West Virginia. The Cheyenne River Indian Reservation in North and South Dakota is larger than Puerto Rico, and the White Earth Indian Reservation is nearly as large as Rhode Island.
On the road to the White Earth Reservation in Minnesota. Jolene Yazzie for Al Jazeera America
“Some of these reservations are millions of acres, and their law enforcement resources are stretched pretty thin,” Ellis noted. You’ve got a handful of officers trying to cover a large land base, which is a tremendous challenge.” Dr. Susan Karol, the IHS’ chief medical officer, agreed, saying, “Our highly rural locations make it hard for treatment to occur.”
Still, she is in favor of naloxone use.
“The fact that you can give naloxone at the scene immediately and then transport the individual from there to the next available facility actually saves you that hour or two it takes to get the individual from wherever they’re found to a medical facility for further care,” she said.
Another challenge facing the proposed delivery system is how little government funding is allocated to Indian Country. Congress sets funding for the BIA, and from 2014 to 2015, money for public safety and justice in Indian country increased from nearly $326 million to just over $328 million, with almost half of that allocated to criminal investigations and police services. Native Americans make up 0.9 percent of the U.S. population, or 2.9 million people. To put that into perspective, Chicago has a population of 2.7 million, and the Chicago Police Department has a budget of $1.2 billion.
“Additional funding from Congress, additional officers on the street would definitely enhance the program,” said Addington.
Harm reduction worker Ashley Martin-Stevens meets with Triina. Jolene Yazzie for Al Jazeera America
For some health experts, including Clinton Alexander, the program director of the Minnesota-based harm reduction program Sacred Spirits, a big-picture law enforcement strategy would also rethink approaches to addiction and arrest so that drug users wouldn’t have to fear police.
“If you and I are shooting up and you overdose and I know that cops are coming, then I’m out of there,” he said, referring to the fact that somebody found under the influence of drugs could be subject to criminal charges. “That’s what most people are doing. And if we’re waiting for law enforcement to administer [naloxone], that’s not effective. They’re not going to get there before they stop completely breathing.”
“I do want to quit, and I am going to quit. I just don’t know when,” says Triina.Jolene Yazzie for Al Jazeera America
Until a broader solution is forged, Alexander and other harm-reduction volunteers carry naloxone with them in order to fill the gaps between police and paramedics.
On the White Earth Reservation, the ancient rice beds and wetlands lay white under a winter sky. Triina unzipped her jacket as she walked into a bar, ordered a cup of coffee and walked slowly to the smoking section.
“What the fuck am I going to do when I sober up?” she said, wiping her nose. “I can’t imagine life right now because I’ve been gone for so fucking long. I honestly don’t even know how I would feel about wanting to feel my real emotions right now or anything like that.”
She sniffled. She had run out of cocaine, and a small, empty plastic bag lay on the table alongside a small mirror and a makeshift straw. She didn’t have enough money for a shot of heroin, but the day was still young. For now, drug use is a full-time job for her, and until she finds a way out, the specter of overdose is always close.
“I could be doing something better,” said Triina. “But I have fucking zero willpower.”
Share This:
Dismiss
Error
Sorry, your comment was not saved due to a technical problem. Please try again later or using a different browser.










Error
Sorry, your comment was not saved due to a technical problem. Please try again later or using a different browser.